 develop on teeth, the acids produced gradually dissolve the enamel, followed by the dentin. Eventually, if left untreated, the lesion may reach the pulp and cause an abscess. (credit: modification of work by “BruceBlaus”/Wikimedia Commons)")
Despite the presence of saliva and the mechanical forces of chewing and eating, some microbes thrive in the mouth. These microbes can cause damage to the teeth and can cause infections that have the potential to spread beyond the mouth and sometimes throughout the body.
Cavities of the teeth, known clinically as dental caries, are microbial lesions that cause damage to the teeth. Over time, the lesion can grow through the outer enamel layer to infect the underlying dentin or even the innermost pulp. If dental caries are not treated, the infection can become an abscess that spreads to the deeper tissues of the teeth, near the roots, or to the bloodstream.
Tooth decay results from the metabolic activity of microbes that live on the teeth. A layer of proteins and carbohydrates forms when clean teeth come into contact with saliva. Microbes are attracted to this food source and form a biofilm called plaque. The most important cariogenic species in these biofilms is Streptococcus mutans. When sucrose, a disaccharide sugar from food, is broken down by bacteria in the mouth, glucose and fructose are produced. The glucose is used to make dextran, which is part of the extracellular matrix of the biofilm. Fructose is fermented, producing organic acids such as lactic acid. These acids dissolve the minerals of the tooth, including enamel, even though it is the hardest material in the body. The acids work even more quickly on exposed dentin ([link]). Over time, the plaque biofilm can become thick and eventually calcify. When a heavy plaque deposit becomes hardened in this way, it is called tartar or dental calculus ([link]). These substantial plaque biofilms can include a variety of bacterial species, including Streptococcus and Actinomyces species.
 Tartar (dental calculus) is visible at the bases of these teeth. The darker deposits higher on the crowns are staining. (b) This tooth shows only a small amount of visible decay. (c) An X-ray of the same tooth shows that there is a dark area representing more decay inside the tooth. (d) Removal of a portion of the crown reveals the area of damage. (e) All of the cavity must be removed before filling. (credit: modification of work by “DRosenbach”/Wikimedia Commons)")
Some tooth decay is visible from the outside, but it is not always possible to see all decay or the extent of the decay. X-ray imaging is used to produce radiographs that can be studied to look for deeper decay and damage to the root or bone ([link]). If not detected, the decay can reach the pulp or even spread to the bloodstream. Painful abscesses can develop.
To prevent tooth decay, prophylactic treatment and good hygiene are important. Regular tooth brushing and flossing physically removes microbes and combats microbial growth and biofilm formation. Toothpaste contains fluoride, which becomes incorporated into the hydroxyapatite of tooth enamel, protecting it against acidity caused by fermentation of mouth microbiota. Fluoride is also bacteriostatic, thus slowing enamel degradation. Antiseptic mouthwashes commonly contain plant-derived phenolics like thymol and eucalyptol and/or heavy metals like zinc chloride (see Using Chemicals to Control Microorganisms). Phenolics tend to be stable and persistent on surfaces, and they act through denaturing proteins and disrupting membranes.
Regular dental cleanings allow for the detection of decay at early stages and the removal of tartar. They may also help to draw attention to other concerns, such as damage to the enamel from acidic drinks. Reducing sugar consumption may help prevent damage that results from the microbial fermentation of sugars. Additionally, sugarless candies or gum with sugar alcohols (such as xylitol) can reduce the production of acids because these are fermented to nonacidic compounds (although excess consumption may lead to gastrointestinal distress). Fluoride treatment or ingesting fluoridated water strengthens the minerals in teeth and reduces the incidence of dental caries.
If caries develop, prompt treatment prevents worsening. Smaller areas of decay can be drilled to remove affected tissue and then filled. If the pulp is affected, then a root canal may be needed to completely remove the infected tissues to avoid continued spread of the infection, which could lead to painful abscesses.
In addition to damage to the teeth themselves, the surrounding structures can be affected by microbes. Periodontal disease is the result of infections that lead to inflammation and tissue damage in the structures surrounding the teeth. The progression from mild to severe periodontal disease is generally reversible and preventable with good oral hygiene.
Inflammation of the gums that can lead to irritation and bleeding is called gingivitis. When plaque accumulates on the teeth, bacteria colonize the gingival space. As this space becomes increasingly blocked, the environment becomes anaerobic. This allows a wide variety of microbes to colonize, including Porphyromonas, Streptococcus, and Actinomyces. The bacterial products, which include lipopolysaccharide (LPS), proteases, lipoteichoic acids, and others, cause inflammation and gum damage ([link]). It is possible that methanogenic archaeans (including Methanobrevibacter oralis and other Methanobrevibacter species) also contribute to disease progression as some species have been identified in patients with periodontal disease, but this has proven difficult to study.123 Gingivitis is diagnosed by visual inspection, including measuring pockets in the gums, and X-rays, and is usually treated using good dental hygiene and professional dental cleaning, with antibiotics reserved for severe cases.

Over time, chronic gingivitis can develop into the more serious condition of periodontitis ([link]). When this happens, the gums recede and expose parts of the tooth below the crown. This newly exposed area is relatively unprotected, so bacteria can grow on it and spread underneath the enamel of the crown and cause cavities. Bacteria in the gingival space can also erode the cementum, which helps to hold the teeth in place. If not treated, erosion of cementum can lead to the movement or loss of teeth. The bones of the jaw can even erode if the infection spreads. This condition can be associated with bleeding and halitosis (bad breath). Cleaning and appropriate dental hygiene may be sufficient to treat periodontitis. However, in cases of severe periodontitis, an antibiotic may be given. Antibiotics may be given in pill form or applied directly to the gum (local treatment). Antibiotics given can include tetracycline, doxycycline, macrolides or β-lactams. Because periodontitis can be caused by a mix of microbes, a combination of antibiotics may be given.
 Healthy gums hold the teeth firmly and do not bleed. (b) Gingivitis is the first stage of periodontal disease. Microbial infection causes gums to become inflamed and irritated, with occasional bleeding. (c) In periodontitis, gums recede and expose parts of the tooth normally covered. (d) In advanced periodontitis, the infection spreads to ligaments and bone tissue supporting the teeth. Tooth loss may occur, or teeth may need to be surgically removed. (credit: modification of work by “BruceBlaus”/Wikimedia Commons)")
When certain bacteria, such as Prevotella intermedia, Fusobacterium species, and Treponema vicentii, are involved and periodontal disease progresses, acute necrotizing ulcerative gingivitis or trench mouth, also called Vincent's disease, can develop. This is severe periodontitis characterized by erosion of the gums, ulcers, substantial pain with chewing, and halitosis ([link]) that can be diagnosed by visual examination and X-rays. In countries with good medical and dental care, it is most common in individuals with weakened immune systems, such as patients with AIDS. In addition to cleaning and pain medication, patients may be prescribed antibiotics such as amoxicillin, amoxicillin clavulanate, clindamycin, or doxycycline.
")
Good oral health promotes good overall health, and the reverse is also true. Poor oral health can lead to difficulty eating, which can cause malnutrition. Painful or loose teeth can also cause a person to avoid certain foods or eat less. Malnutrition due to dental problems is of greatest concern for the elderly, for whom it can worsen other health conditions and contribute to mortality. Individuals who have serious illnesses, especially AIDS, are also at increased risk of malnutrition from dental problems.
Additionally, poor oral health can contribute to the development of disease. Increased bacterial growth in the mouth can cause inflammation and infection in other parts of the body. For example, Streptococcus in the mouth, the main contributor to biofilms on teeth, tartar, and dental caries, can spread throughout the body when there is damage to the tissues inside the mouth, as can happen during dental work. S. mutans produces a surface adhesin known as P1, which binds to salivary agglutinin on the surface of the tooth. P1 can also bind to extracellular matrix proteins including fibronectin and collagen. When Streptococcus enters the bloodstream as a result of tooth brushing or dental cleaning, it causes inflammation that can lead to the accumulation of plaque in the arteries and contribute to the development of atherosclerosis, a condition associated with cardiovascular disease, heart attack, and stroke. In some cases, bacteria that spread through the blood vessels can lodge in the heart and cause endocarditis (an example of a focal infection).
As noted earlier, normal oral microbiota can cause dental and periodontal infections. However, there are number of other infections that can manifest in the oral cavity when other microbes are present.
As described in Viral Infections of the Skin and Eyes, infections by herpes simplex virus type 1 (HSV-1) frequently manifest as oral herpes, also called acute herpes labialis and characterized by cold sores on the lips, mouth, or gums. HSV-1 can also cause acute herpetic gingivostomatitis, a condition that results in ulcers of the mucous membranes inside the mouth ([link]). Herpetic gingivostomatitis is normally self-limiting except in immunocompromised patients. Like oral herpes, the infection is generally diagnosed through clinical examination, but cultures or biopsies may be obtained if other signs or symptoms suggest the possibility of a different causative agent. If treatment is needed, mouthwashes or antiviral medications such as acyclovir, famciclovir, or valacyclovir may be used.
 This cold sore is caused by infection with herpes simplex virus type 1 (HSV-1). (b) HSV-1 can also cause acute herpetic gingivostomatitis. (credit b: modification of work by Klaus D. Peter)")
The yeast Candida is part of the normal human microbiota, but overgrowths, especially of Candida albicans, can lead to infections in several parts of the body. When Candida infection develops in the oral cavity, it is called oral thrush. Oral thrush is most common in infants because they do not yet have well developed immune systems and have not acquired the robust normal microbiota that keeps Candida in check in adults. Oral thrush is also common in immunodeficient patients and is a common infection in patients with AIDS.
Oral thrush is characterized by the appearance of white patches and pseudomembranes in the mouth ([link]) and can be associated with bleeding. The infection may be treated topically with nystatin or clotrimazole oral suspensions, although systemic treatment is sometimes needed. In serious cases, systemic azoles such as fluconazole or itraconazole (for strains resistant to fluconazole), may be used. Amphotericin B can also be used if the infection is severe or if the Candida species is azole-resistant.
")
The viral disease mumps is an infection of the parotid glands, the largest of the three pairs of salivary glands ([link]). The causative agent is mumps virus (MuV), a paramyxovirus with an envelope that has hemagglutinin and neuraminidase spikes. A fusion protein located on the surface of the envelope helps to fuse the viral envelope to the host cell plasma membrane.
Mumps virus is transmitted through respiratory droplets or through contact with contaminated saliva, making it quite contagious so that it can lead easily to epidemics. It causes fever, muscle pain, headache, pain with chewing, loss of appetite, fatigue, and weakness. There is swelling of the salivary glands and associated pain ([link]). The virus can enter the bloodstream (viremia), allowing it to spread to the organs and the central nervous system. The infection ranges from subclinical cases to cases with serious complications, such as encephalitis, meningitis, and deafness. Inflammation of the pancreas, testes, ovaries, and breasts may also occur and cause permanent damage to those organs; despite these complications, a mumps infection rarely cause sterility.
Mumps can be recognized based on clinical signs and symptoms, and a diagnosis can be confirmed with laboratory testing. The virus can be identified using culture or molecular techniques such as RT-PCR. Serologic tests are also available, especially enzyme immunoassays that detect antibodies. There is no specific treatment for mumps, so supportive therapies are used. The most effective way to avoid infection is through vaccination. Although mumps used to be a common childhood disease, it is now rare in the United States due to vaccination with the measles, mumps, and rubella (MMR) vaccine.
")
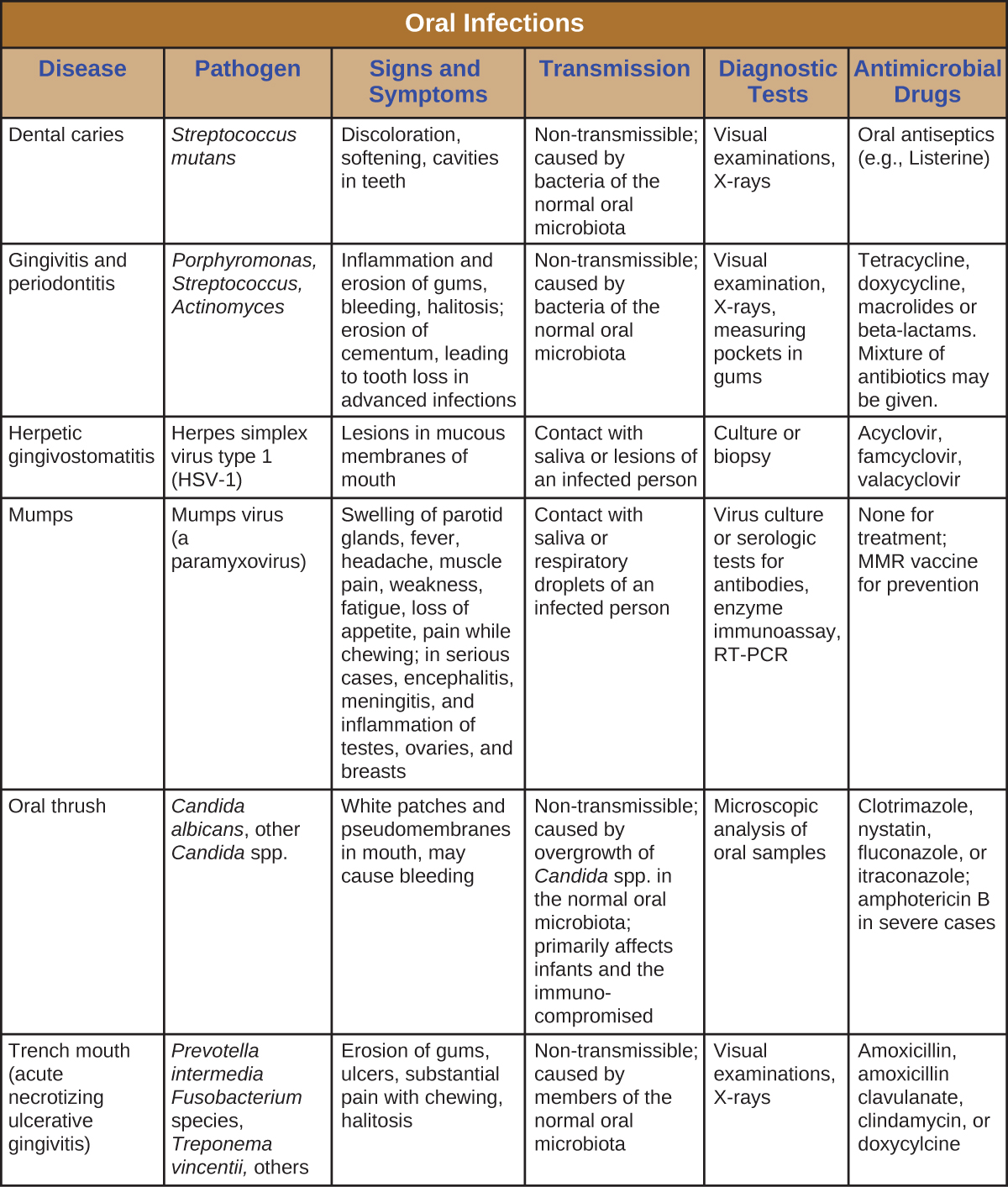
Infections of the mouth and oral cavity can be caused by a variety of pathogens, including bacteria, viruses, and fungi. Many of these infections only affect the mouth, but some can spread and become systemic infections. [link] summarizes the main characteristics of common oral infections.
What pathogen is the most important contributor to biofilms in plaque?
B
What type of organism causes thrush?
C
In mumps, what glands swell to produce the disease’s characteristic appearance?
C
Which of the following is true of HSV-1?
B
When plaque becomes heavy and hardened, it is called dental calculus or _________.
tartar
Why do sugary foods promote dental caries?

You can also download for free at http://cnx.org/contents/e42bd376-624b-4c0f-972f-e0c57998e765@5.3
Attribution: